United Healthcare Release Of Information Form
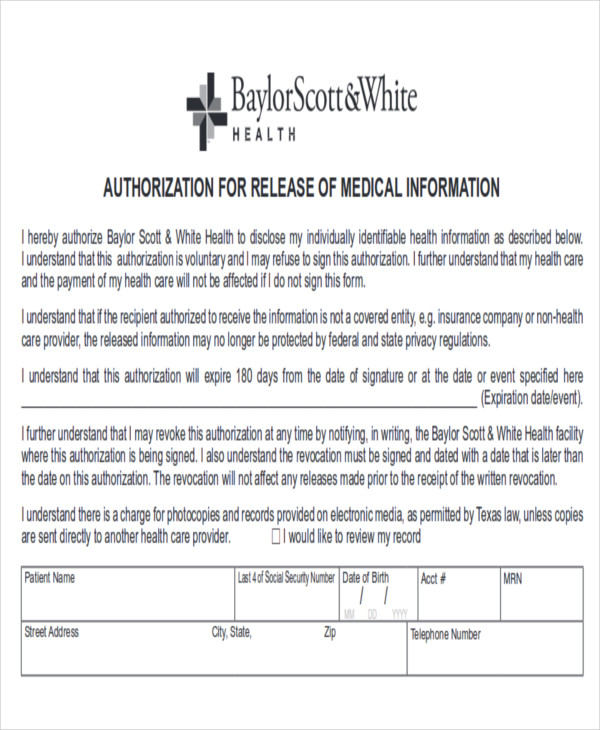
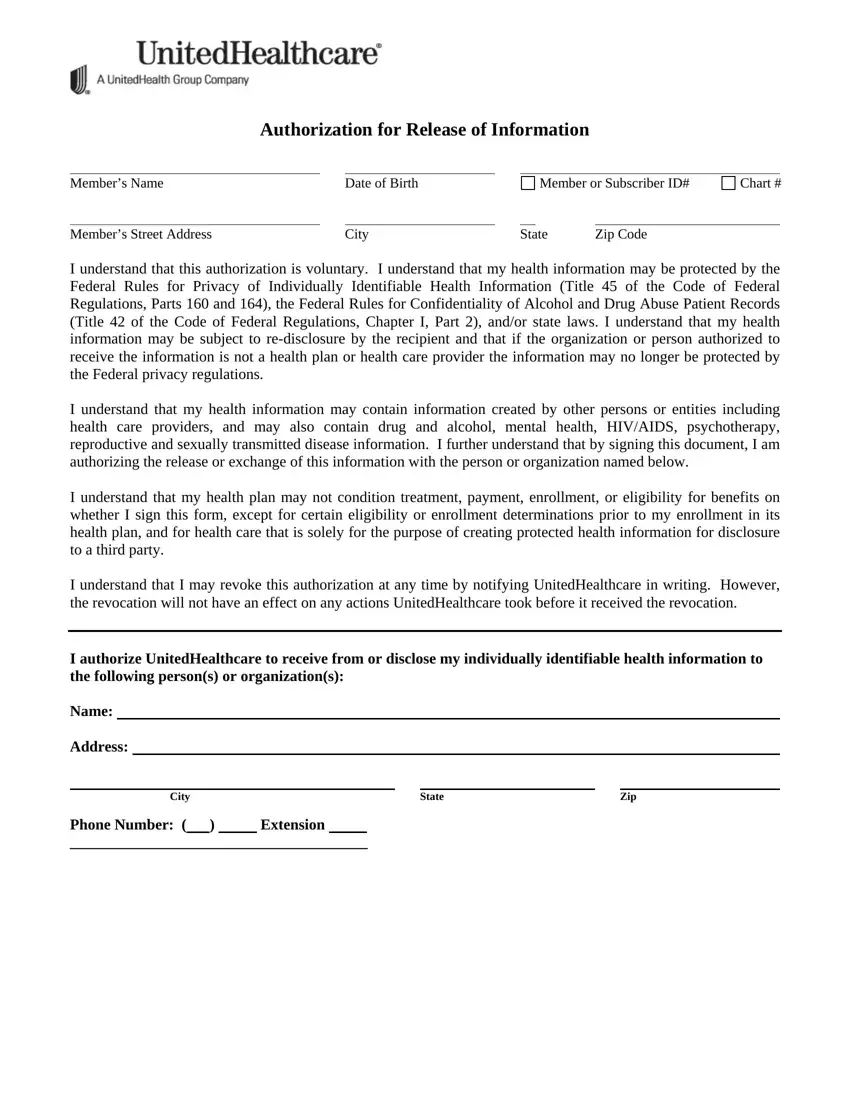
United Healthcare Release Of Information Form - I authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following. Must be completed for all authorizations: I authorize disclosure of all my health information, including information relating to medical, pharmacy, dental, vision, mental health,. Complaint forms are available at hhs.gov/ocr/office/file/index.html. This form allows you to authorize unitedhealthcare and its affiliates to disclose your health information to a person or. If you speak english, language. I may revoke this authorization at any time by notifying unitedhealthcare in writing; I hereby authorize the use or disclosure of my. Authorization for release of information section a: Fill out this form to give unitedhealthcare and its affiliates permission to share your personal information with others based on your.
If you speak english, language. Fill out this form to give unitedhealthcare and its affiliates permission to share your personal information with others based on your. I may revoke this authorization at any time by notifying unitedhealthcare in writing; Authorization for release of information section a: Must be completed for all authorizations: I hereby authorize the use or disclosure of my. Complaint forms are available at hhs.gov/ocr/office/file/index.html. I authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following. I authorize disclosure of all my health information, including information relating to medical, pharmacy, dental, vision, mental health,. This form allows you to authorize unitedhealthcare and its affiliates to disclose your health information to a person or.
Authorization for release of information section a: If you speak english, language. I authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following. However, the revocation will not have an effect on any. I hereby authorize the use or disclosure of my. Must be completed for all authorizations: Complaint forms are available at hhs.gov/ocr/office/file/index.html. I may revoke this authorization at any time by notifying unitedhealthcare in writing; This form allows you to authorize unitedhealthcare and its affiliates to disclose your health information to a person or. I authorize disclosure of all my health information, including information relating to medical, pharmacy, dental, vision, mental health,.
Insurance Release Form Template
This form allows you to authorize unitedhealthcare and its affiliates to disclose your health information to a person or. I authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following. Complaint forms are available at hhs.gov/ocr/office/file/index.html. Fill out this form to give unitedhealthcare and its affiliates permission to share your personal information.

Free Medical Release Form Templates Word PDF DocFormats
Authorization for release of information section a: I authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following. If you speak english, language. View the links below to find member forms you can download, making it quicker to take action on claims, reimbursements and more. I hereby authorize the use or disclosure.

Authorization to Release Healthcare Information Download the free
Must be completed for all authorizations: View the links below to find member forms you can download, making it quicker to take action on claims, reimbursements and more. I hereby authorize the use or disclosure of my. However, the revocation will not have an effect on any. I authorize unitedhealthcare and its affiliates to receive from or disclose my individually.

Mental Health Release Of Information Form Pdf Fill Online, Printable
I may revoke this authorization at any time by notifying unitedhealthcare in writing; Fill out this form to give unitedhealthcare and its affiliates permission to share your personal information with others based on your. View the links below to find member forms you can download, making it quicker to take action on claims, reimbursements and more. Complaint forms are available.

Automate Authorization to release medical information Document
Authorization for release of information section a: View the links below to find member forms you can download, making it quicker to take action on claims, reimbursements and more. Fill out this form to give unitedhealthcare and its affiliates permission to share your personal information with others based on your. I may revoke this authorization at any time by notifying.

The extraordinary Medical Release Form Template 30+ Medical Release
I may revoke this authorization at any time by notifying unitedhealthcare in writing; Must be completed for all authorizations: I authorize disclosure of all my health information, including information relating to medical, pharmacy, dental, vision, mental health,. View the links below to find member forms you can download, making it quicker to take action on claims, reimbursements and more. Authorization.
United Healthcare Release Of Information PDF Form FormsPal
I authorize disclosure of all my health information, including information relating to medical, pharmacy, dental, vision, mental health,. I hereby authorize the use or disclosure of my. I authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following. Must be completed for all authorizations: If you speak english, language.

Save time and money on Medical information release form paperwork
If you speak english, language. I may revoke this authorization at any time by notifying unitedhealthcare in writing; Complaint forms are available at hhs.gov/ocr/office/file/index.html. I authorize disclosure of all my health information, including information relating to medical, pharmacy, dental, vision, mental health,. However, the revocation will not have an effect on any.
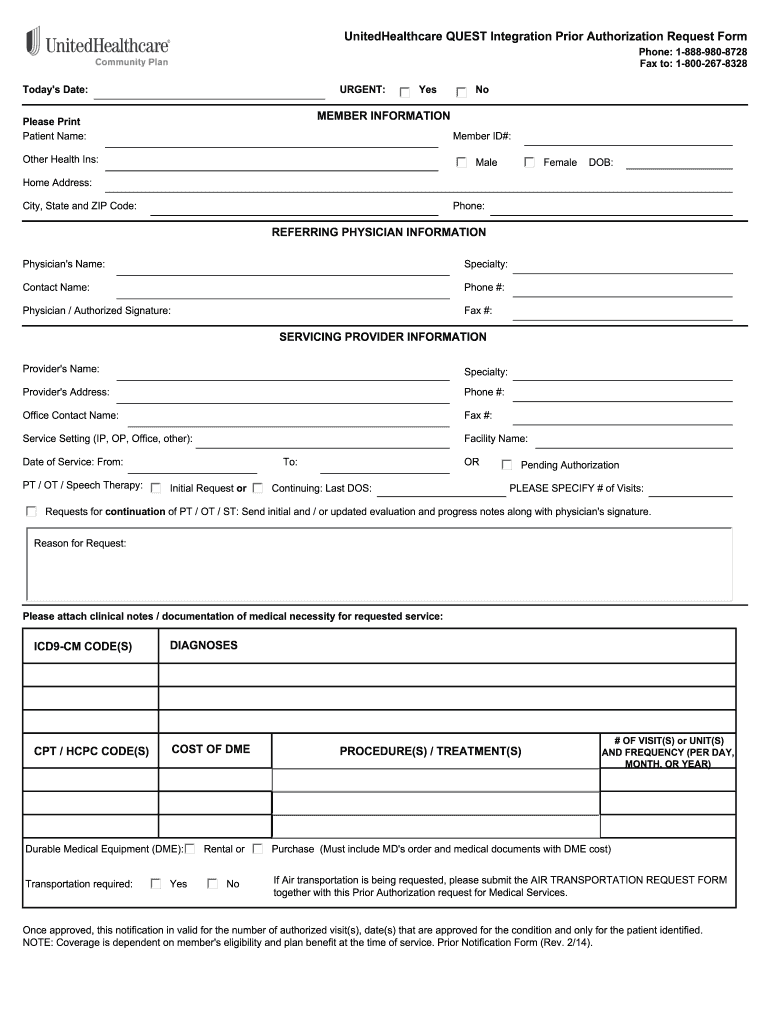
United healthcare prior authorization form Fill out & sign online DocHub
Must be completed for all authorizations: Complaint forms are available at hhs.gov/ocr/office/file/index.html. I authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following. Authorization for release of information section a: I may revoke this authorization at any time by notifying unitedhealthcare in writing;
United Healthcare Release Of Information PDF Form FormsPal
However, the revocation will not have an effect on any. Must be completed for all authorizations: I authorize unitedhealthcare and its affiliates to receive from or disclose my individually identifiable health information to the following. This form allows you to authorize unitedhealthcare and its affiliates to disclose your health information to a person or. I hereby authorize the use or.
Fill Out This Form To Give Unitedhealthcare And Its Affiliates Permission To Share Your Personal Information With Others Based On Your.
I may revoke this authorization at any time by notifying unitedhealthcare in writing; Must be completed for all authorizations: Complaint forms are available at hhs.gov/ocr/office/file/index.html. If you speak english, language.
I Authorize Unitedhealthcare And Its Affiliates To Receive From Or Disclose My Individually Identifiable Health Information To The Following.
However, the revocation will not have an effect on any. Authorization for release of information section a: View the links below to find member forms you can download, making it quicker to take action on claims, reimbursements and more. I hereby authorize the use or disclosure of my.
This Form Allows You To Authorize Unitedhealthcare And Its Affiliates To Disclose Your Health Information To A Person Or.
I authorize disclosure of all my health information, including information relating to medical, pharmacy, dental, vision, mental health,.