Psychotropic Medication Consent Form
Psychotropic Medication Consent Form - Each resident’s drug/medication regimen is managed and monitored to help stabilize or. Psychiatric medication consent forms purpose: • targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. If i take this medication. To provide clinical policy guidelines for obtaining the beneficiary/client’s informed consent to receive. Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a.
Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a. Psychiatric medication consent forms purpose: Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. If i take this medication. Each resident’s drug/medication regimen is managed and monitored to help stabilize or. • targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): To provide clinical policy guidelines for obtaining the beneficiary/client’s informed consent to receive.
Psychiatric medication consent forms purpose: • targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a. To provide clinical policy guidelines for obtaining the beneficiary/client’s informed consent to receive. Each resident’s drug/medication regimen is managed and monitored to help stabilize or. Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. If i take this medication.
Medication Consent Form 2024
• targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. If i take this medication. To provide clinical policy guidelines for obtaining the beneficiary/client’s informed consent to receive. Psychiatric medication consent forms purpose:
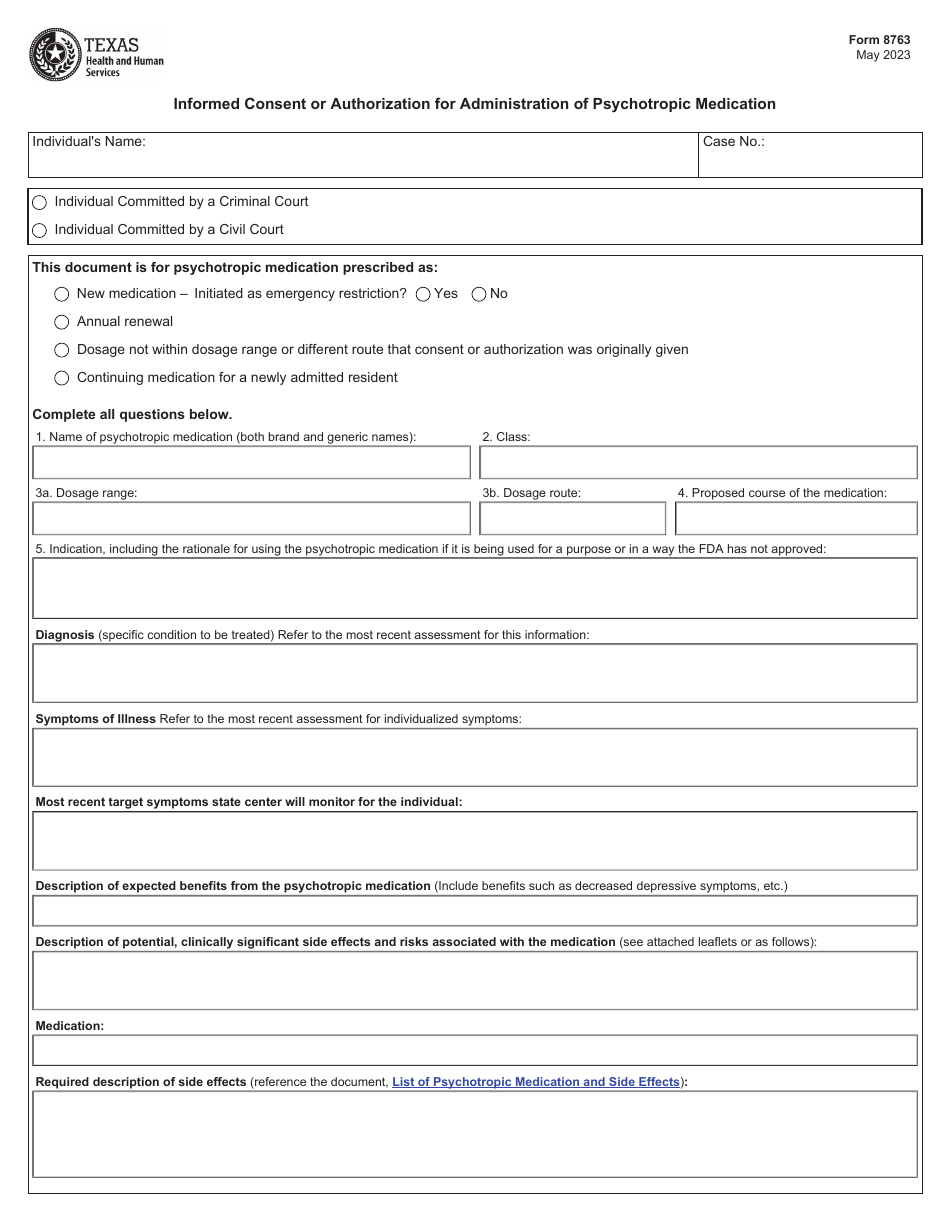
Form 8763 Fill Out, Sign Online and Download Fillable PDF, Texas
Psychiatric medication consent forms purpose: • targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): Each resident’s drug/medication regimen is managed and monitored to help stabilize or. Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a. If i take this medication.

Psychotropic Medication Consent CF 0173 C 1/15. Psychotropic Medication
• targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): If i take this medication. Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a. Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental.
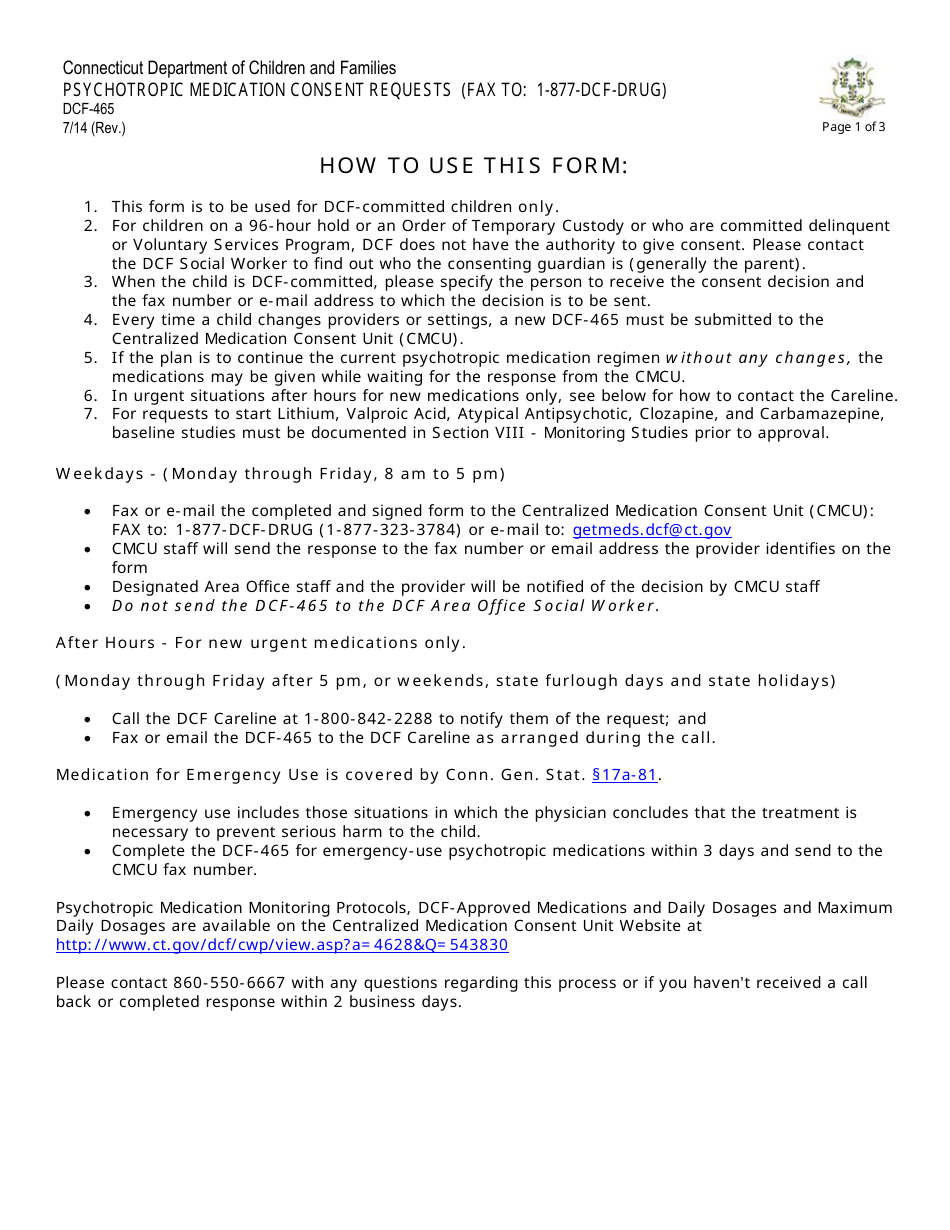
Form DCF465 Fill Out, Sign Online and Download Fillable PDF
Psychiatric medication consent forms purpose: Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. To provide clinical policy guidelines for obtaining the beneficiary/client’s informed consent to receive. • targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): Informed consent is the process in.
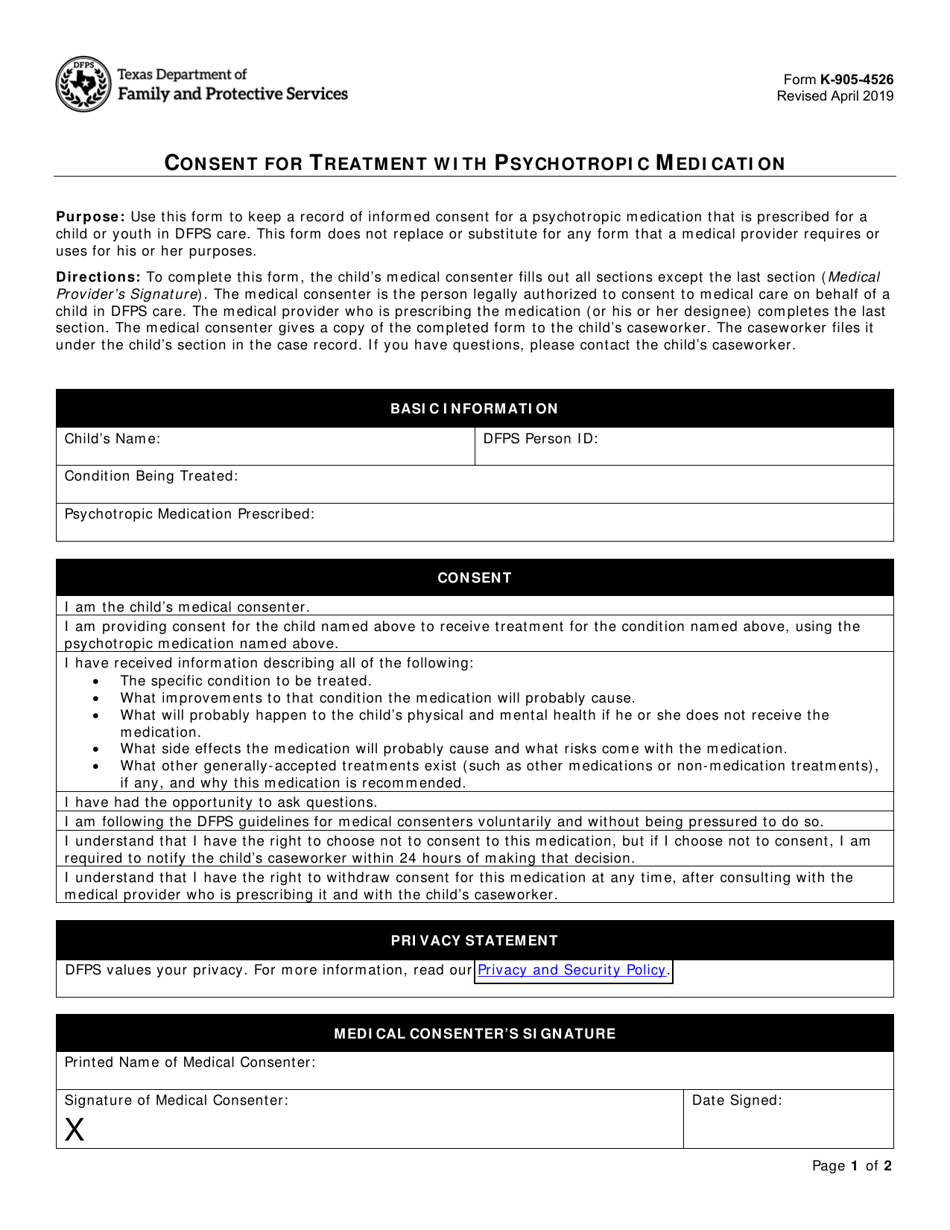
Form K9054526 Fill Out, Sign Online and Download Fillable PDF
Psychiatric medication consent forms purpose: If i take this medication. Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. • targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): To provide clinical policy guidelines for obtaining the beneficiary/client’s informed consent to receive.
Psychotropic Medication Informed Consent DIGITAL FORM
• targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a. Psychiatric medication consent forms purpose: If i take this medication. Understand that my psychiatrist will prescribe, and i will take this medication as.
Fillable Form Cfs 431A Psychotropic Medication Request Form
Each resident’s drug/medication regimen is managed and monitored to help stabilize or. Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. If i take this medication. • targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): To provide clinical policy guidelines for obtaining.

Informed Consent Form For Psychotropic Medications 2022 Printable
To provide clinical policy guidelines for obtaining the beneficiary/client’s informed consent to receive. If i take this medication. Psychiatric medication consent forms purpose: • targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): Each resident’s drug/medication regimen is managed and monitored to help stabilize or.

Dhs Psychotropic Medication Consent Form 2024 Printable Consent Form 2022
Psychiatric medication consent forms purpose: Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. If i take this medication. Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a. Each resident’s drug/medication regimen is managed and.

Fillable Online SCARC, Inc. Psychotropic Medication Consent Form Fax
Each resident’s drug/medication regimen is managed and monitored to help stabilize or. If i take this medication. • targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)): Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. Psychiatric medication consent forms purpose:
To Provide Clinical Policy Guidelines For Obtaining The Beneficiary/Client’s Informed Consent To Receive.
Understand that my psychiatrist will prescribe, and i will take this medication as a part of my mental health treatment program. Informed consent is the process in which a health care provider educates a patient about the risks, benefits, and alternatives of a. Each resident’s drug/medication regimen is managed and monitored to help stabilize or. If i take this medication.
Psychiatric Medication Consent Forms Purpose:
• targeted symptoms (signs and symptoms identified by the prescriber for treatment with psychotropic medication(s)):